
Polymer valves refined through computer simulations aim to reduce costs and improve minimally invasive procedures.
Aortic stenosis occurs when the heart’s aortic valve does not open fully as a result of calcified aortic valve disease (CAVD). CAVD is caused by calcium buildup in the valve and can lead to heart failure. The condition affects more than 2.5 million people over the age of 75 in the US.1 For years, the valves have been replaced through open heart surgery: surgical aortic valve replacement (SAVR). Increasingly, however, older patients who cannot tolerate surgery have been treated with a minimally invasive procedure: transcatheter aortic valve replacement (TAVR), in which a new valve compressed in a catheter is guided through a blood vessel and expanded over the diseased valve.
As the TAVR procedure and the design of TAVR valves continue to be improved, more doctors and patients are opting for TAVR instead of surgery because the minimally invasive nature of the procedure allows for a drastically reduced recovery time. Recovery from SAVR takes several months, while TAVR patients typically leave the hospital and can function normally within a few days.
However, the increased use of TAVR in younger patients raises a serious question about the durability of the valves, as they are now expected to function for many more years in patients’ bodies. Longer-term studies of TAVR procedures have identified potential degeneration and leak problems with the tissue valves currently used for TAVR.
Led by NIBIB Fellow Danny Bluestein, Ph.D., Professor of Biomedical Engineering at Stony Brook University, New York, a team of experts in blood flow dynamics in the cardiovascular system has designed and laboratory-tested an experimental polymer TAVR valve. The group hopes that the use of polymers will overcome some of the problems with long-term use of tissue valves, improving the procedure and outcomes so that it can be reliably offered to more patients of all ages, reducing the need for open heart surgery.
“We can test the valves in the early stages of development using computer models and with mechanical devices that mimic the heart pumping blood through the valve,” Bluestein said. “Our test systems and computer simulations allow us to evaluate a polymer valve and identify specific structural problems that affect performance. We can then make necessary changes, for example to the shape, flexibility or other aspects of the polymer that would mitigate the problems and increase efficiency.”
Bluestein explained that a key advantage of working with polymers is that, unlike fabrics, their shape and properties can be changed, allowing problems with the devices to be rectified before moving on to costly animal testing.
Adds Grace Peng, Ph.D., director of the NIBIB program in Mathematical Modeling, Simulation and Analysis: “Dr. Bluestein and his colleagues have been pioneers in combining mathematical models and experimental techniques to design and make real-world improvements in devices used to treat cardiovascular disorders. Their work is an excellent example of how mathematical modeling and simulation approaches can accelerate the development and increase the reliability of treatments and medical devices that save the lives of thousands of patients with serious illnesses.”
Testing the new polymer TAVR valve
The valve prototype was developed in collaboration between Stony Brook University and Polynova Cardiovascular Inc., Stony Brook, NY. The valve is a TAVR version of a Polynova polymeric valve designed for surgical aortic valve replacement (SAVR). The valve was made by placing raw polymer pellets into a mold under heat and pressure for one hour using compression molding. The ability to make valves from molds would allow for mass production and reduced costs compared to animal tissue valves.
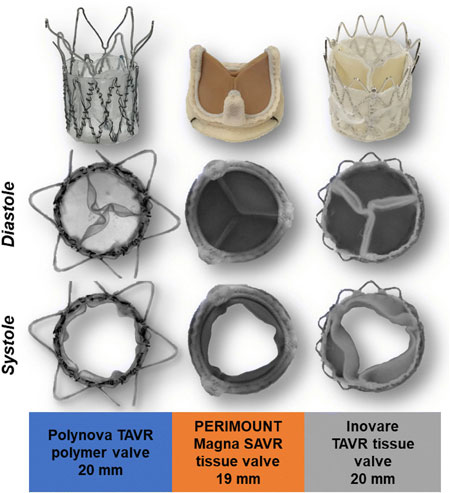
The experimental Polynova valve was compared to tests of two valves currently used in patients, the Perimount SAVR used in open heart surgery and the Inovare TAVR used in the minimally invasive procedure. Both are animal tissue valves. The hydrodynamic tests evaluated how the valves function when simulated blood fluid is pumped through them at the same rate as the heartbeat.
In the baseline test, liquid was pumped through the valves to see how well they opened. The size of the opening when the fluid is pumped is called the effective orifice area (EOA). A large EOA, as well as a more rounded one, indicates the best performance. The EOA of the polymer valve was larger and more rounded than the SAVR and TAVR tissue valves.
For the second test, the valves were mounted on a 3D-printed model of a real patient’s aorta. “Patient-specific models are reconstructed from CT scans of TAVR candidates, using custom computer algorithms,” Bluestein said. “The reconstructed anatomy is then used to simulate TAVR deployment, as well as advanced computational fluid dynamics studies on this ‘virtual patient.’ We will then be able to identify potential problem areas that will inform redesign to optimize valve performance.”
In both tests, changes in the pressure of the fluid as it passed through each valve were measured. For all three valves, performance decreased slightly in the patient-specific test compared to the mechanical device used in the first test. This is to be expected because variation in patient anatomy places varying pressures on all valves, resulting in shape changes and slightly less efficient flow. However, there were only slight differences between the valves in terms of performance in both test environments, which were negligible.
The final test measured the activation of platelets as they flow through each valve. Platelets are small vesicles in the blood that cause clots to form when activated. The Bluestein group has focused on developing implanted valves and heart pumps designed to reduce clotting. These implants can cause disturbances in blood flow that activate platelets and initiate the coagulation cascade, increasing the formation of blood clots and the risk of stroke.
Because of this risk, doctors must routinely prescribe these patients permanent anticoagulant medications to prevent dangerous clotting events. However, blood thinners have their disadvantages, including prolonged bleeding before wounds heal and, in the worst cases, the possibility of hemorrhagic strokes. Therefore, the goal of creating devices with a reduced tendency to clot decreases the need for long-term anticoagulant treatment.
The results of the coagulation tests indicated that the polymer valve was the least likely to activate platelets.
“We believe these initial tests of polymer TAVR are quite promising, as performance was similar and often better than tissue valves in this hemodynamic study,” Bluestein said. The group is currently testing other aspects of the valve, including durability, stability during and after compression in the catheter that positions the valve (known as crimping), and susceptibility to the buildup of calcium deposits, which is the leading cause of aortic valve disease.
The work was published in the January 2019 issue of Annals of Biomedical Engineering.2.
This project was supported by Quantum Prize Phase II-U01EB012487 from the National Institute of Biomedical Imaging and Bioengineering, grant STTR R41-HL134418 from the National Heart, Lung, and Blood Institute, and the Center for Biotechnology: a New York State Advanced Technology Center, New York State Department of Economic Development.
1.Ramaraj R, Sorrell V. Degenerative aortic stenosis. BMJ 2008;336:550-5.


